)
Social determinants are a far larger factor in someone’s health than the quality and amount of health care they receive. An individual’s employment status, wellbeing, living conditions and income all have a greater impact on their health than the accessibility and quality of care provided by health services.
As the biggest employer in England and a significant economic force in local communities, the NHS has a unique opportunity to use its resources to influence the wellbeing of the population it serves and reduce the health inequalities that exist in England.
Introduction
Last year the Health Foundation published a report on how the NHS could embrace some of these opportunities by acting as an anchor institution. Currently, there is no internationally agreed definition of an anchor institution, but the Health Foundation defined such institutions as ‘large, public sector organisations that are unlikely to relocate and have a significant stake in a geographical area… they have sizable assets that can be used to support local community wealth building and development through procurement and spending power, workforce and training and buildings and land’.
Health care organisations in other countries are exploring this idea, for example, the Montefiore system in New York and Canterbury in New Zealand. In some areas of England, including Preston, Leeds, Birmingham and Greater Manchester, the NHS is exploring ways of using its influence as a large employer to change the economic status of local populations. But this approach is currently the exception rather than the norm, although the long- term plan does make a specific commitment to explore how the NHS can take on this role more often in the future.
We hope that this long read will help people working in the NHS to understand the level of economic influence their organisations can have and the benefits this can bring to local populations, in a way they may not have considered before.
Why do we consider only NHS provider organisations?
This is an introductory, high-level analysis of the economic role of the NHS, and we have restricted our analysis to NHS provider organisations, as these account for most NHS spending and so make a good starting point for discussion. Economic impact of NHS spending in the Black Country provides an example of a full estimate of the economic value of the NHS.
This analysis focuses on NHS spending and does not cover social care or public health, but it should be possible to create similar estimates of relative wages or per cent of people employed in these sectors using different data sources, for example, Skills for Care’s adult social care workforce dataset.
Methodology
We have brought data on economic activity within the wider economy together with data on employment and wages in the NHS at sustainability and transformation partnership (STP) area, as this geography most closely reflects the population level most relevant to the role of the anchor institution (pending the full establishment of integrated care systems (ICSs)). A fuller explanation of the methodology is provided below.
This long read looks at the NHS’s role within the wider economy from several perspectives – the level of influence the NHS holds through employment and spending; the relative level of earnings in the NHS compared to the wider local economy; and the provision of training, skills and opportunity.
What proportion of local employment is with NHS providers?
It’s important to understand the context in which the NHS, as an employer, sits. We don’t have data on employment by organisation in each local area, but we can use data in the Labour Force Survey (LFS) to provide comparisons across industries. In most regions in England, the two biggest industries are retail and wholesale trade, and health and social care provision (including private sector). Across England as a whole, health and social care provides 12 per cent of all employment (the LFS includes all health and social care roles, not just the NHS provider trust roles included in our analysis). The only other industry to account for more than 10 per cent of employment nationally is the retail sector.
The NHS is the largest employer in England, but the proportion of the local market occupied by NHS provider organisations varies across STPs (see Figure 1).
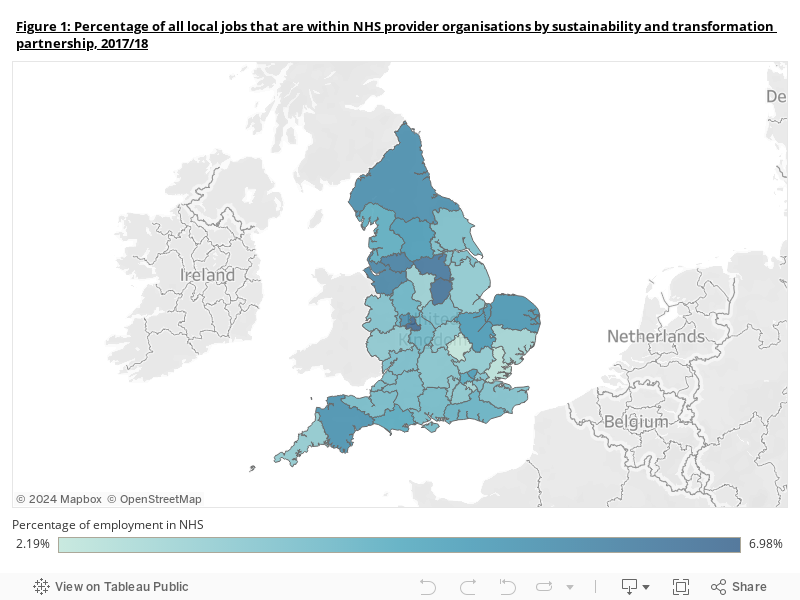
In some areas, NHS providers make up a relatively small percentage of total employment, especially in south-east England, where, in areas like Bedfordshire, Luton and Milton Keynes, and Mid and South Essex, the NHS employs slightly more than 2 per cent of all people employed locally. In contrast, in areas like Birmingham and Solihull, and in Nottingham and Nottinghamshire close to 7 per cent of all people in employment work within NHS provider organisations.
Although much of the past 10 years has been marked by the implementation of pay restraint, the NHS can offer opportunities and economic security for its staff, especially in areas where there has been a reduction in economic opportunity. The NHS offers reliable, stable employment: it is not going to withdraw from an area at scale, even if local services are realigned, making it uniquely positioned to provide economic opportunity at a time when the employment rate has never been higher and more uncertain in nature.
The NHS’s connection to its local economy
We should also consider the indirect impact the NHS can have on connected local businesses. By buying from local suppliers, and being a responsible partner, NHS organisations can help others provide economic opportunity to local people. As part of the Health Foundation’s report, the Centre for Local Economic Strategies calculated that nearly 70 per cent of Leeds Teaching Hospitals Trust’s spending on procured goods and services went to companies operating outside the wider local area. There may be opportunities for some of this spending to be redirected locally – for example, organisations in Preston have been working on restructuring their spending with a focus on local suppliers and have since moved from spending £37.5 million locally in 2012 to £135 million in 2017, creating 1,700 jobs.
The creation of local enterprise partnerships and local industrial strategies across England is, as NHS Confederation has pointed out, a significant opportunity for NHS organisations to become more involved with the economic development of their local region. There is no ideal level of local investment and investing all money locally is unrealistic and undesirable (as increased costs for suppliers could raise prices if required to work locally instead of at scale). Instead, given the link between employment and health outcomes, ICSs and STPs could think about how NHS organisations in their area can sustainably invest in local businesses, while protecting efficiency, to influence health at the population level.
Relative wages
By plotting the median annual earnings for staff working in NHS provider organisations on a map (see Figure 2), we can see that there is a very different pattern in how much people earn working for the NHS compared with the overall economy in each STP area (see Figure 3).

Note: data represents salary per headcount member of staff, not full-time equivalent.
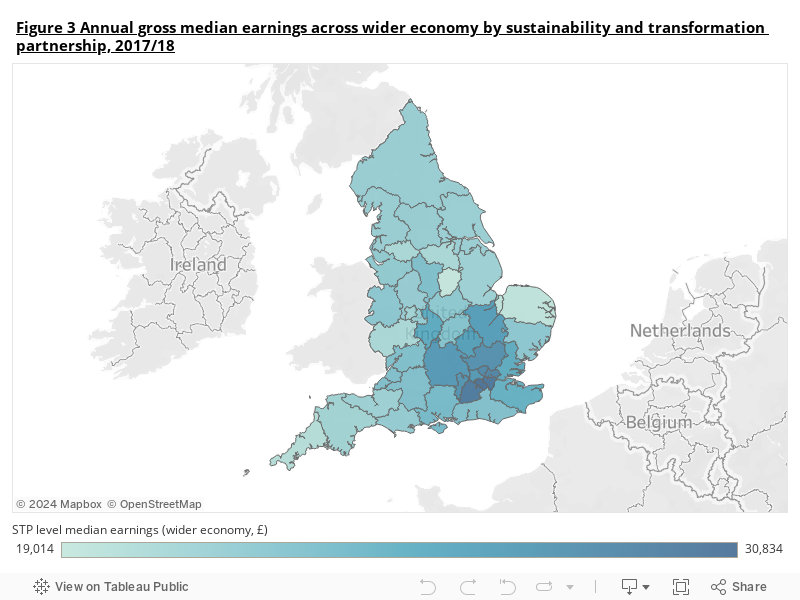
There is more variance in wages across the wider economy than within the NHS (see Figure 3). This is what we would expect to see because most staff working in the NHS provider sector are contracted within a nationally agreed pay deal, Agenda for Change (AfC). However, there are some significant differences in how much an individual working for the NHS earns depending on which region they work in. In London, for example, wages are at least £4,600 a year more, on average, than outside London, a result of an uplift built into staff pay under AfC. However, outside London there is still almost £6,000 difference in the median amount earned by NHS staff in different areas (£28,047 in Joined Up Care Derbyshire compared to £22,132 in Humber, Coast and Vale STP). Theoretically, there should be little variation across regions, given the national pay deal, although there is some flexibility to address local recruitment and retention difficulties. One possible explanation for the variation we are seeing could be a concentration of local staff at the lower or higher pay points of their band.
These figures only cover earnings for roles in the NHS provider sector; including the commissioning sector and roles in subcontracted organisations would produce different figures. Working patterns in the NHS, where part-time working and shift-working are common, are likely to be different to patterns in other sectors. Our figures on earnings include full-time and part-time workers. Industries with a higher number of part-time roles are likely to pay less in total earnings to staff (on average, total earnings for the retail sector are lower and those in manufacturing are higher than in the NHS, for example).
If we look at the relationship between the ratio of NHS earnings relative to the wider local economy and income deprivation within STPs, we can see that as the proportion of people living in income deprivation rises, the amount earned on average in NHS provider organisations increases.
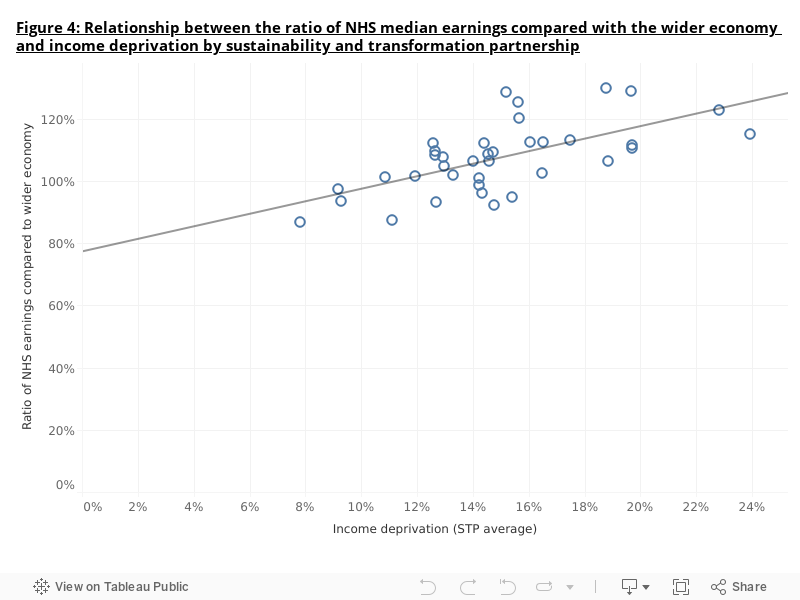
In some areas people working in the wider economy have higher average earnings that those working in the NHS, but this usually occurs in areas where people have unusually high average earnings, such as Surrey or Buckinghamshire. Nationally, on average, employees in the NHS provider sector earn 7.3 per cent more than workers do on average in the wider economy. The largest difference between NHS and wider economy earnings is seen in Nottinghamshire, where on average an NHS provider sector employee earns 30 per cent more than the average worker in the wider local economy.
One of the key features of an ‘anchor institution’ is to act as a leader in terms of local employment. Many anchor institutions regard their pay levels as an investment in their local area, money that will be spent locally to improve conditions for local businesses and encourage economic growth. Given the importance of income in determining health, the financial rewards and job security that working in the NHS offer are an opportunity for health systems to influence population health.
Investing in skills and opportunity for people
We should not just focus on how much the NHS spends on people and supplies. As the Royal Society for the encouragement of Arts, Manufactures and Commerce highlighted in 2016, many areas in England underwent significant industrial change in the 1970s and 1980s, concentrating job opportunities in regional urban centres and creating inequalities in economic opportunity that have not been properly addressed since. In this context, it is even more important for NHS organisations to support their local economies to improve growth and help address the health inequalities that are so closely linked to economic inequality.
The NHS cannot redress all those shifts alone, but by partnering with other organisations locally and working at scale themselves, NHS organisations can provide opportunities to their own staff and people living in their local areas. While the NHS has little flexibility locally to adjust wages, there is much more flexibility with recruitment and training and some NHS provider organisations are already taking advantage of this. Local NHS providers can access central funding, as well as their own organisational budgets, to offer training and continuing personal development opportunities for their staff, allowing them to develop within and beyond their day-to-day roles and improve their skills. Apprenticeships are also being increasingly offered as a first step into work, and the NHS has historically provided bursaries to nursing and medical students.
An important role of anchor institutions is to invest in skills and training for local communities, which also benefits organisations themselves through a better skilled and more effective workforce, but NHS providers are being left without the funding needed to provide this. As we have pointed out before, investment in training in the NHS has been falling, from 5 per cent of total health spending in 2006/07 to slightly more than 3 per cent in 2018/19. According to the NHS Staff Survey, the proportion of staff receiving any training, learning or development in the past 12 months (other than mandatory training) has been flat over the past 4 years – at 73 per cent in 2015 and 71 per cent in 2018 – so there is plenty of potential for more staff to undertake additional training. The Chancellor announced an increase of £150 million in Health Education England’s budget in the 2019 Spending Round, the first increase in 6 years.
NHS England’s full People Plan, due later this year, will be an opportunity for the NHS to make a renewed commitment to providing opportunities for professional development for NHS staff and people living in areas with limited economic opportunity who could benefit financially and in terms of wellbeing from the job security and professional standards that the NHS can offer.
Some examples of NHS organisations investing in skills and local opportunities for local people can be seen in the Health Foundation’s work: Leeds Teaching Hospitals Trust has partnered with Leeds City Council to target career opportunities towards communities in the most deprived local areas; Bart’s Health NHS Trust has a proportion of roles reserved for local candidates identified by the local council; and University Hospitals Birmingham has partnered with The Prince’s Trust to establish a learning hub – a purpose-built centre that offers ‘pre-employment advice, training, guidance and direct links to jobs in the NHS to unemployed local people and those furthest from the labour market’.
Conclusion
The NHS is often talked about as the biggest employer in England, but thinking at this scale can overlook the local importance of the NHS in areas with higher levels of deprivation. In these areas the NHS is a key employer, providing good terms and conditions and opportunities for high-quality, professional work, and contributing to the local economy by investing in the region and in training and education for staff.
The NHS can use its national and local roles together to create sustainable employment for local communities that helps develop the local skill-base and affects the root causes of ill health and health inequality. To continue to miss that opportunity at a time when health at the population level has never been more important would be disappointing. The move towards ICSs gives the NHS the chance to take new and innovative steps to reduce health inequalities and affect the economic determinants of health in a way it has never done before.
What can England and Singapore learn from each other?
This study will examine the barriers and enablers to transformative change in population health, prevention, and primary and community care across a number of different settings.
Report calls for country to embark on collective 'national mission for ageing' to manage challenges and opportunities of an older society
A new report by The King's Fund and International Longevity Centre UK urges England to adopt a national mission for ageing, learning from Japan and Sweden to prioritise prevention and he...
Healthy ageing: what can England learn from Japan and Sweden about meeting the challenge of an ageing society?
Demographic ageing is one of the most important challenges facing developed countries in the 21st century. How England can respond to these challenges, particularly in terms of its healt...
)
From evidence to impact: making prevention stick
The UK’s health is in trouble, and it’s holding us back. Prevention can help – but is often sidelined when pressure mounts. Join us to explore how to keep progress going when the system ...
Comments